What Is a Surgically Assisted Rapid Palatal Expander?
One of the most common procedures in orthodontics for children and teenagers is palatal expansion (maxillary expansion). Orthodontists use expanders to eliminate posterior crossbites, reduce crowding, and broaden the overall width of an arch. Expansion in orthodontics can be classified into two categories, dental and skeletal.
Dental expansion only moves the teeth, not the underlying bone
Dental expansion occurs when the teeth move outward to create an arch that is bigger than before treatment. In the front of the mouth, dental expansion moves teeth forward. In the back of the mouth, the teeth move sideways. If only the crown of the tooth (the top part of the tooth that is out of the gums) is expanded, the movement is called “tipping.” If both the crown and root are moved together, we call this “bodily movement.” If the teeth are moved beyond the size of the supporting tissues, they can actually be pushed right out of the bone causing recession and even loss of the teeth (known as dehiscence at the top of the root and fenestration lower on the root).
Skeletal expansion actually moves the palatal bone
Skeletal expansion occurs when the two halves of the palate (which are separate bones) are physically separated by the expander. Theoretically, the arch is expanded because only the bones are moved and the position of the teeth is not affected. Because the bones are moved apart and the teeth are attached to them, it is common for patients to develop a space between the two front teeth. This is one sign that patients and orthodontists can use to determine which type of expansion is occurring.
The growth status of the palatal suture determines type of expansion
The primary factor that determines whether an expander produces dental or skeletal movement is the status of the palatal growth plate or “mid-palatal suture.” If the suture is not fused, a palatal expander will separate the two sides of the palate as the width of the arch is increased. If the growth plate is fused, the expander will still widen the arch, but the movement will be primarily dental in nature (tipping) and a space will not appear between the two front teeth. Although there are variations of normal, the mid-palatal suture is typically fused in female patients by age 15 in girls and 17 in boys.
Surgery may be required to expand the palate after growth is complete
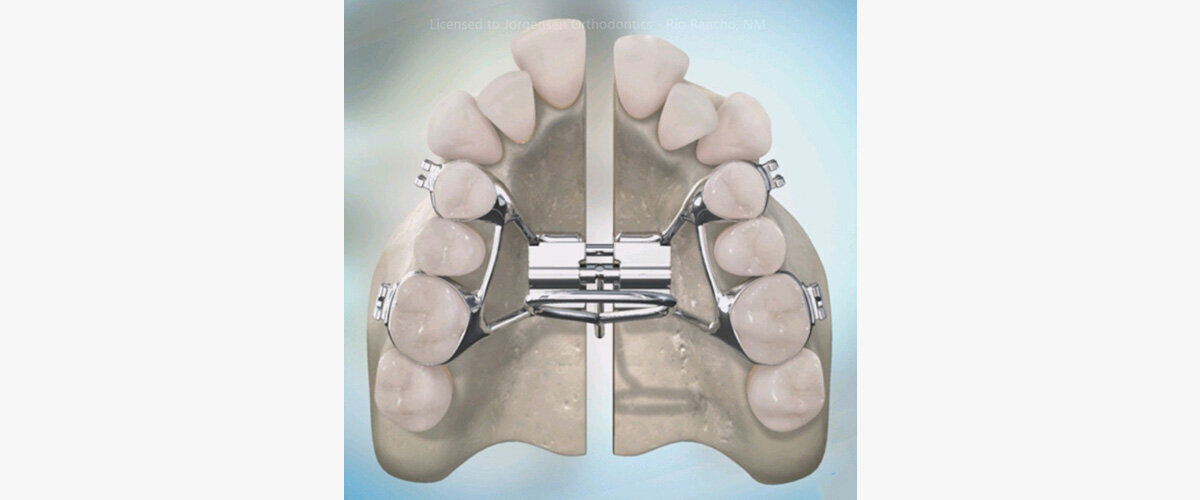
Posterior crossbites, crowding, and narrow arch forms are also problems for adult patients. While dental expansion can be achieved with an expander (as well as with standard orthodontic wires), the amount is limited by the size of the supporting bone. When skeletal expansion is required in an adult, the use of a palatal expander must be accompanied by a surgical procedure to re-open the fused suture. This is known as a SARPE or SARME (Surgically Assisted Rapid Palatal Expander or Surgically Assisted Rapid Maxillary Expander).
This surgery is performed under the upper lip so that no exterior scars are created. During the procedure, an oral surgeon creates precision cuts in the bone right above the roots of the teeth and down the middle of the palate. Over the next few weeks, the patient will be required to slowly activate the expander until the desired width is achieved. The expansion is done slowly to allow the overlying gum tissues to stretch and accommodate the new width. Because the bones are separated in surgically assisted cases, a space is always created between the front teeth. After expansion is achieved, the expander must remain in the mouth for several months to allow the bone to heal. Once healed, upper braces can be placed and the teeth moved into their desired positions.
NOTE: The author, Dr. Greg Jorgensen, is a board-certified orthodontist who is in the private practice of orthodontics in Rio Rancho, New Mexico (a suburb on the Westside of Albuquerque). He was trained at BYU, Washington University in St. Louis, and the University of Iowa in the United States. Dr. Jorgensen’s 25 years of specialty practice and nearly 10,000 finished cases qualify him an expert in two-phase treatment, extraction and non-extraction therapy, functional orthodontics, clear aligners (Invisalign), and multiple bracket systems (including conventional braces, Damon and other self-ligating brackets, Suresmile, and lingual braces). This blog is for informational purposes only and is designed to help consumers understand currently accepted orthodontic concepts. It is not a venue for debating alternative treatment theories. Dr. Jorgensen is licensed to diagnose and treat patients only in the state of New Mexico. He cannot diagnose cases described in comments nor can he select treatment plans for readers. Please understand that because he has over 40,000 readers each month, IT IS IMPOSSIBLE FOR HIM TO RESPOND TO EVERY QUESTION. Please read all of the comments associated with each article as most of the questions he receives each week have been asked and answered previously. The opinions expressed here are protected by copyright laws and can only be used with written permission from the author.